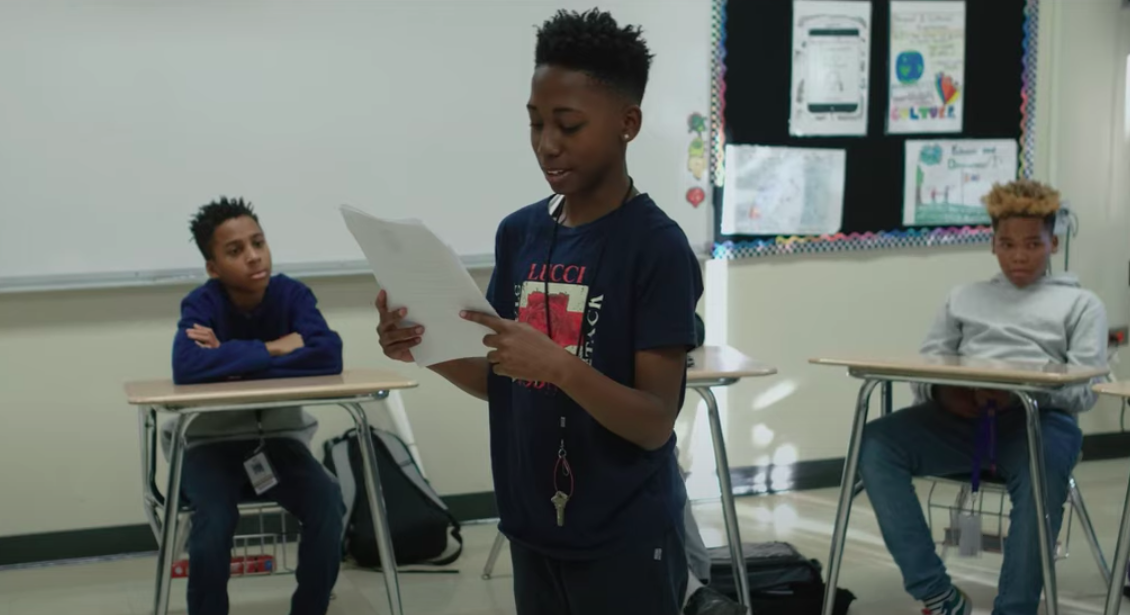
After School
M.E.P. takes place on site at Brooks & Julian Middle Schools. Students join mentors, junior mentors, and staff for one-on-one & group mentoring, homework help, life-skills workshops, exploration workshops, and recreational activities.
SCHEDULE:
Julian Middle School
3rd Floor (B-wing)
Monday & Tueday
3:30-5:30 pm
Brooks Middle School
3rd Floor (C-wing)
Wednesday & Thursday
3:30-5:30 pm
Mentoring Empowerment Program
GRADES 6-8
Enroll Your Student.